Physical Therapy ERA Reconciliation: Why Getting Paid Isn't the Same as Getting Paid Correctly
ERA reconciliation errors cost PT practices more than most realize. Learn how unmatched payments quietly drain your practice's revenue.
Your billing team submitted the claims. The payer processed them. The payment landed in your account. Most billing managers consider that a clean close. But ERA reconciliation — the step that confirms your practice actually received what it was owed — is where a surprising amount of PT revenue quietly disappears. And because money keeps arriving, the gap often goes unnoticed for months.
What ERA Reconciliation Actually Is
When an insurance company processes a claim, they generate an Electronic Remittance Advice — an ERA, or 835 file — explaining exactly how they handled each line item. Paid at contracted rate. Adjusted for deductible. Denied with CO-4. Reduced under CO-45. It's the official record of what they're paying and why.
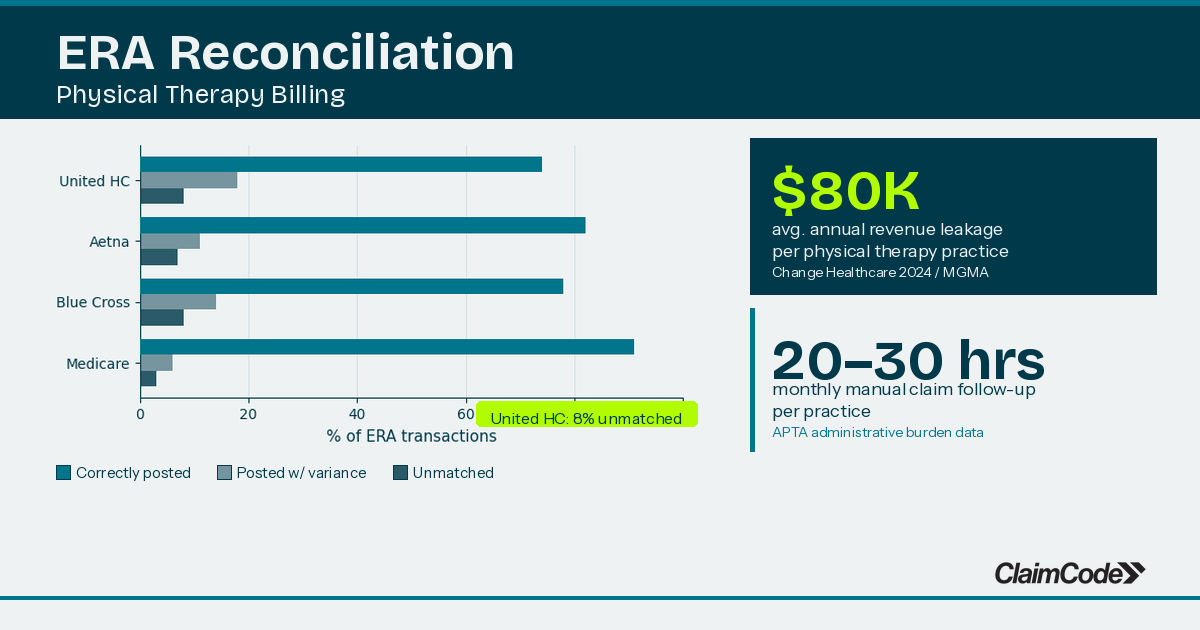
ERA reconciliation is the process of matching that file against your bank deposits and your practice management system to confirm three things are aligned: what you submitted, what the payer said they paid, and what actually cleared your account.
In theory it's straightforward. In practice, it's one of the most consistently skipped steps in PT billing — because when revenue keeps flowing, it's easy to assume it's flowing correctly.
Three Places ERA Reconciliation Breaks Down
Contractual underpayments posted without review. Payers occasionally reimburse below your contracted rate — sometimes due to payer error, sometimes because a fee schedule was updated without notification. If ERA posting is manual or semi-automated, catching these discrepancies requires someone to check each payment line against your negotiated rates. Most practices don't have a systematic workflow for this. The underpayment gets posted, accepted, and never recovered.
Denial codes that don't trigger a follow-up workflow. An ERA denial for CO-97 (bundling) requires a different response than CO-4 (late submission) or CO-16 (claim information incomplete). When denials get posted to your system without routing to a specific follow-up action, they sit. They age. And eventually they fall outside the timely filing window. Industry data shows that 47.5% of denied claims are never resubmitted — not because billing teams gave up, but because there's no reliable system for tracking which denials still need action (Change Healthcare, 2024).
Batch deposits that don't trace back to individual claims. Many clearinghouses consolidate multiple ERAs into a single ACH deposit. Reconciling that deposit back to individual claim payments is a manual matching task. For a practice running 400+ claims per month across multiple providers and payers, this reconciliation often happens monthly — or quarterly — or not at all. The result: persistent uncertainty about whether specific claims were actually paid.
What This Costs at Scale
The financial impact of poor ERA reconciliation compounds quickly. The average PT practice carries a 15–20% denial rate (MGMA/HFMA, 2024). For a 6-provider practice billing at standard rates, that denial exposure translates to roughly $199,980 in uncollected revenue annually — and that figure doesn't account for contractual variance errors that never register as denials in the first place.
The billing managers we talk to describe a consistent pattern: the ERA queue gets processed, but exception management — what to do with claims that weren't paid correctly — is where things fall apart. There simply isn't enough time to be systematic about it when one person is managing billing across multiple providers and locations.
The problem isn't lack of effort. It's lack of visibility.
What Good ERA Reconciliation Looks Like
Practices with clean ERA workflows share a few consistent habits.
They map denial codes to follow-up actions before those denials ever reach a queue. CO-97 triggers a rebilling workflow. CO-4 triggers a timely filing review. CO-45 triggers a documented write-off. The response is predetermined, not improvised claim by claim.
They review contractual variance on a weekly cycle, not monthly. Any ERA payment that falls below the contracted rate by more than a defined threshold gets flagged before the deposit closes. This catches both payer errors and fee schedule mismatches while they're still actionable.
They track denial patterns at the payer level, not just the claim level. If a specific payer is consistently underpaying on CPT 97110, that's a contract issue worth escalating — not a one-off error to fix and move on. The difference between catching a pattern and absorbing it indefinitely is whether you have aggregate visibility across payers and CPT codes.
The Visibility Gap Most Billing Tools Don't Solve
Most PT practice management systems handle claim submission and basic ERA posting reasonably well. What they don't provide is an analytics layer that surfaces underpayment patterns across payers, flags denial codes that have gone unworked past a threshold, or shows how your reconciliation performance compares to practices your size.
That visibility gap is what drives the "we're probably leaving money on the table but we can't see where" frustration that billing managers describe. ClaimCode's physical therapy billing intelligence is built to address that gap — sitting alongside your existing EHR and clearinghouse to give your team the data needed to catch ERA errors before they become permanent losses.
If you're not sure what ERA reconciliation gaps might be costing your practice, the ClaimCode ROI Calculator lets you estimate your revenue exposure based on provider count and current denial rate.
Related Reading
Denied Outpatient Claims Rose 14% in 2025. Here's What That Costs the Average PT or Chiro Practice.
Denied outpatient claim amounts rose 14% in 2025. Here's what the math means for PT and chiro practices — and how to stop the revenue from walking out the door.
What the UHC Prior Auth Expansion Means for Your PT and Chiropractic Billing Team
UHC's Medicare Advantage prior authorization program keeps expanding. Here's what the 6-visit waiver actually covers — and where the documentation traps are.

Dr. Andrew O'DonnellPhD, LSSGB
CEO and founder of ClaimCode. Expert in insurance analytics, digital transformation, and business operations. Passionate about helping private wellness practices manage their revenue cycle with meaningful insights.
Ready to stop losing revenue to denied claims?
ClaimCode gives your billing team real-time claim visibility and AI-powered remediation guidance — at flat-fee pricing.
Get Early Access