ERA Reconciliation for Physical Therapy Practices: What the Data Is Trying to Tell You
Most PT practices post ERA payments without reading the patterns underneath. Here's what your remittance data reveals — and what it's costing you.
Every payment your practice receives from an insurance company arrives with a document most billing teams don't have bandwidth to analyze carefully: the Electronic Remittance Advice (ERA). The gap between receiving ERAs and actually learning from them is costing PT and chiropractic practices real money — and most practices don't realize it.
What an ERA Actually Contains
An Electronic Remittance Advice is the insurance company's transaction-level record of what it paid, what it adjusted, what it denied, and why. For most billing teams, ERA reconciliation means one thing: posting the payment against the correct claim. Payment matches claim, mark it closed, move on.
That's not wrong — but it's only half the job. The other half is pattern analysis: reading across ERAs over time to understand how each payer behaves, which denial reason codes repeat, and whether specific procedure codes or modifiers are generating consistent write-downs. Most practices never get to that second half — not because they don't see the value, but because the transaction volume makes it nearly impossible to do manually.
A 6-provider physical therapy practice processes roughly 1,400 claims per month across multiple payers. Each generates a remittance record. Reconciling them individually is a full-time job. Analyzing the patterns across all of them requires something different.
The Revenue Hidden in Your Remittance Data
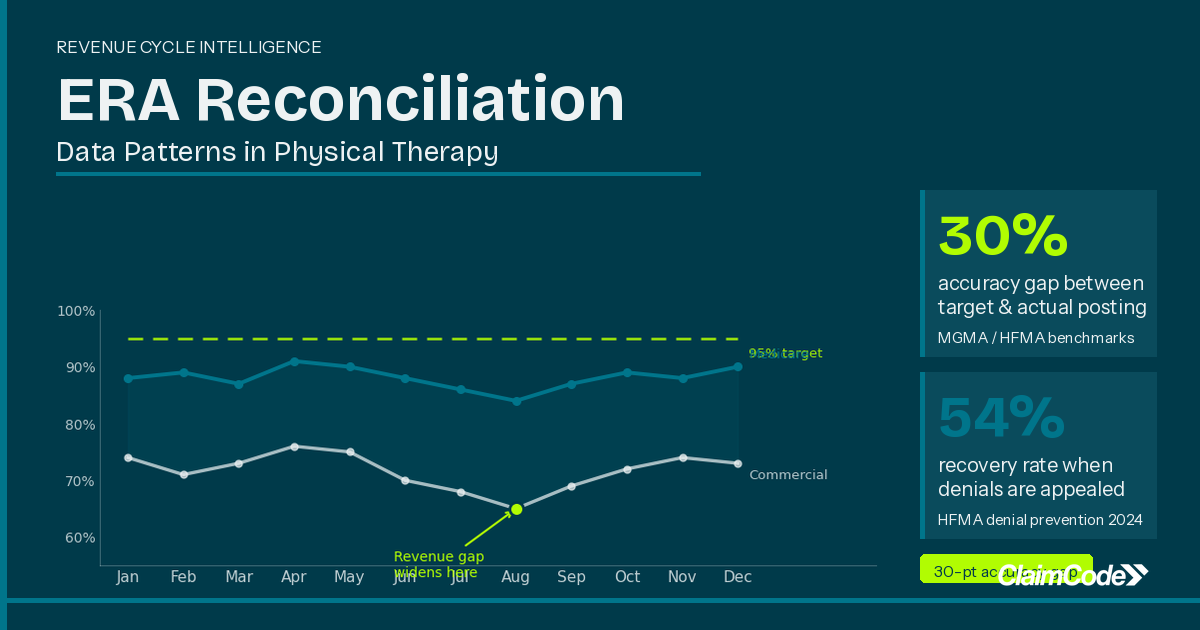
The average PT practice operates with a 15–20% initial claim denial rate, according to MGMA and HFMA 2024 data. That headline number matters — but what matters more is the distribution underneath it.
Not all payers deny at the same rate. Not all procedure codes get denied equally. In most practices, denial rates vary significantly across payers, but billing teams have no easy way to see that variation. They're posting payments and chasing denials reactively, without the pattern visibility to ask: why is Payer A denying this code 18% of the time when Payer B only denies it 4% of the time?
According to Change Healthcare's 2024 analysis, 47.5% of denied claims are never resubmitted. That's not because billing teams have given up — it's because without clear prioritization, there's no way to know which denials are worth pursuing. Small-dollar denials get abandoned because the appeal cost exceeds the recovery. Pattern-driven denials — the same issue repeating across dozens of claims — go unnoticed because no one sees the aggregate.
For a 6-provider practice, the math on abandoned and unrecovered denials adds up to roughly $199,980 in annual revenue leakage, based on CMS 2025 reimbursement data and APTA 2024 visit volume benchmarks (ClaimCode internal model). It's not that the billing team did something wrong. It's that ERA data, on its own, doesn't self-organize into actionable patterns.
What Thorough ERA Reconciliation Looks Like
Most practices define reconciliation as "payment is posted." Thorough ERA analysis goes further: it connects remittance data to original claims in a way that reveals patterns across payers and providers — not just confirms that checks cleared.
Payer-level denial tracking is the starting point. Knowing that one payer denied 17% of your claims last quarter while another denied 6% gives you the diagnostic information to ask why — and whether the fix is in your documentation, your modifier usage, or your appeal process for that specific payer.
Denial reason code aggregation is the next layer. CARC codes — CO-16 ("claim lacks information or has a billing error"), CO-4 ("service not covered by this payer"), CO-97 ("payment adjusted because this service or procedure requires that a qualifying service or procedure be received first") — tell you exactly why a claim was denied. When CO-16 appears consistently for a specific provider or location, that's a documentation training issue, not an appeal issue. The ERA has been telling you that for months.
Write-off pattern analysis matters too. Contractual adjustments are expected. But repeated write-downs beyond your contracted rate — or adjustments applied to procedure codes that shouldn't carry them — are worth catching before they become normalized. ERA data shows them. Most practices don't aggregate across enough claims to spot them.
The Multi-Location Challenge
Practices with multiple locations face an additional layer of complexity: each payer manages claims from each location through its own processes, sometimes with different local policies for prior authorization, modifier requirements, and documentation standards. What generates a denial at your South Shore location may clear without issue at your Boston clinic — for reasons that aren't apparent without cross-location ERA analysis.
Billing managers at growing practices consistently describe the same situation: they're skilled at the transaction work, they know how to appeal, they understand their payers — but they don't have consolidated visibility across all their payer relationships at once. The ERA data is there. It just doesn't arrive organized in a way that surfaces the patterns underneath it.
What Your Billing Team Should Know Every Month
You don't need to overhaul your workflow to start improving your ERA process. Begin with three questions your billing team should be able to answer every month: What is each of your top five payers' denial rate for the past 90 days? What are your three most common denial reason codes across all payers? And which codes are appearing repeatedly from the same payer?
If pulling these answers requires manual cross-referencing or custom report runs, that's a process gap worth addressing. The AMA has found that 54% of denied claims can be successfully recovered when properly appealed — but only when billing teams have the visibility to know which denials to prioritize. Without ERA pattern analysis, you're making those decisions on instinct rather than data.
Making Your ERA Data Work for You
ERA reconciliation isn't a new idea. But treating ERAs as a source of pattern intelligence — rather than just payment confirmation documents — is still uncommon in smaller PT and chiropractic practices. The practices that do it aren't necessarily larger or better-staffed. They've built a system to use the data their payers are already sending them.
ClaimCode analyzes ERA data across payers to surface denial patterns and identify the highest-value recovery opportunities for your billing team, working alongside your existing EHR and clearinghouse without disrupting your current workflow. See how ClaimCode's specialty logic for physical therapy practices handles 8-minute rule validation, modifier 59 bundling, and KX threshold tracking.
To see how much revenue your practice could realistically be recovering, use the ROI Calculator at roi.claimcode.app — input your provider count and average visit volume and it runs the math.
Your payers are already sending you everything you need to recover more revenue. The question is whether your process is set up to read it.
Related Reading
Denied Outpatient Claims Rose 14% in 2025. Here's What That Costs the Average PT or Chiro Practice.
Denied outpatient claim amounts rose 14% in 2025. Here's what the math means for PT and chiro practices — and how to stop the revenue from walking out the door.
What the UHC Prior Auth Expansion Means for Your PT and Chiropractic Billing Team
UHC's Medicare Advantage prior authorization program keeps expanding. Here's what the 6-visit waiver actually covers — and where the documentation traps are.

Dr. Andrew O'DonnellPhD, LSSGB
CEO and founder of ClaimCode. Expert in insurance analytics, digital transformation, and business operations. Passionate about helping private wellness practices manage their revenue cycle with meaningful insights.
Ready to stop losing revenue to denied claims?
ClaimCode gives your billing team real-time claim visibility and AI-powered remediation guidance — at flat-fee pricing.
Get Early Access